Part 3: Estimating your risk of a future fracture due to impaired bone health: Is Fracture Risk Really Age-Dependent?
Authors:
Kimberly Zambito, MD, Orthopaedic Surgeon and Owner of Qualis Os
Dr Nick Birch FRCS (Orth), Consultant Spine and Bone Health Specialist
Andrew Bush, MD, Orthopaedic Surgeon
For decades doctors have known that fracture rates increase as people get older, the primary reason being impaired bone density and bone toughness. As a result, in the 1990s there was a big push to develop screening tools to predict future fracture risk and allow earlier intervention to prevent fractures if a person’s risk was high. Many methods have been developed over the years including FRAX, Q-Fracture, the Osteoporosis Self-Assessment Tool (OST), DXA T- and Z-scores, and more recently REMS T-scores, Z-scores and Fragility Scores.
The simplest of these tools is the OST which uses a formula based on gender, age and weight to estimate whether a person has osteoporosis and by inference, whether their fracture risk is elevated. By definition this tool is age dependent. However, it turns out not to be particularly helpful in predicting future fracture risk as osteoporosis by itself only accounts for about a third of fragility (low trauma) fractures.
A more complicated prediction tool is FRAX which was originally developed in Sheffield, England in the 1990s. It was later adopted by the World Health Organisation as their official fracture prediction device, and it is now the most commonly used screening tool for fragility fracture risk. FRAX works by comparing a person’s characteristics to information about fracture rates in a very large database that matches their age, weight, gender, country of origin and a variety of clinical features. The fracture data from the database was recorded when FRAX was developed and from this matching process a risk profile is generated. Importantly, that data has not been updated in the years since it was first collected and given the change in lifestyles and wellness characteristics that have emerged since the 1990s, it is no longer certain that the matching process used by FRAX is accurate in relation to the current population and FRAX may now be systematically over-estimating future fracture risk.
The clinical risk factors (CRF) in FRAX include a past history of a fracture, history of a parental hip fracture, current use of steroid medication, current smoking and / or heavy drinking plus whether a person has a range of other medical conditions that might lead to impaired bone health e.g. malabsorption in the gut, thyroid disease, long-term liver or kidney disease, diabetes and rheumatoid arthritis. Each CRF adds a certain level of risk to the estimate of how likely a future fracture is. So, a person would reasonably expect to have a low FRAX risk if they remain healthy and active even in to their 70s and 80s. Not so! It turns out that FRAX is highly age dependent which means that however healthy you are, your risk when using FRAX to estimate fracture risk inexorably increases as you age.
Initially, FRAX was derived to determine fracture risk without input from diagnostic densitometry (DXA). Subsequently, an algorithm was developed that allowed DXA-derived BMD values, or T-scores, for the hip to be included in the fracture risk estimate (REMS-derived BMD values cannot currently be used in FRAX calculations). This goes some way to improve the estimate as it uses real data from the person being assessed rather than just comparing that person to broad categories of physiological features. Trabecular Bone Score (TBS) is a DXA method that was developed to estimate bone toughness in the spine and TBS values can now be included in FRAX as well. The addition of these values increases the accuracy of fracture risk prediction via FRAX, but the age bias remains.
This blog focuses on how increasing age affects FRAX generated fracture risk, irrespective of how healthy you are, and how this might lead to medical decision-making that might not make much sense.
Let’s explore the use of FRAX in prediction of fragility fracture risk. FRAX can be found on the internet at https://frax.shef.ac.uk/FRAX/.
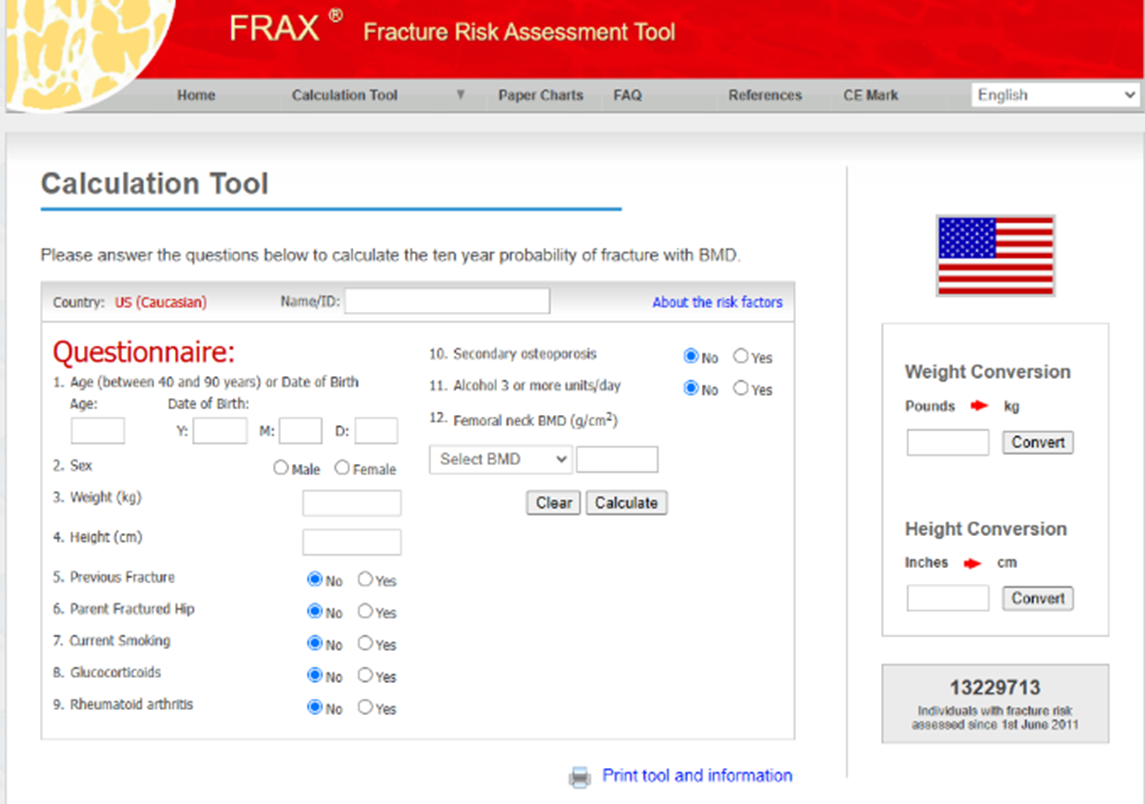
FRAX estimates fracture risk by using demographic information (Questions 1 - 4) and Yes / No responses for the clinical risk factors (Questions 5 – 11). The 12th entry is T-score or bone mineral density values if a person has had a DXA scan. After the questions are answered, FRAX calculates the likelihood that a fracture will occur in the next 10 years. The results are presented as two percentages – the percent chance of Major Osteoporotic Fractures (MOF: fractures in the upper limb, spine and lower limb) and the percent chance of Hip Fractures. Treatment algorithms for osteoporosis recommend medical intervention when the value of the MOF risk is 20% or higher and when the hip fracture risk is 3% or higher. It is because of the treatment algorithms that your physician may recommend medical treatment of osteoporosis.
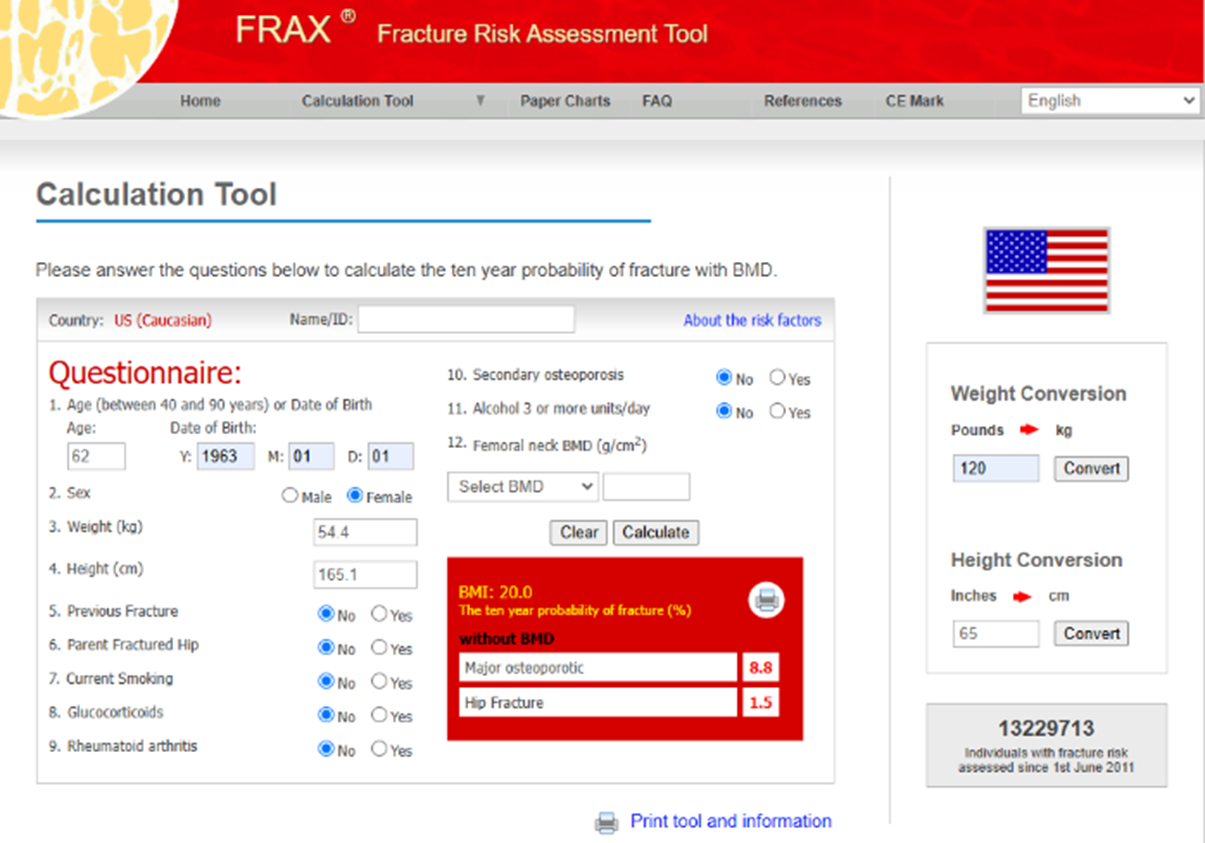
The FRAX questionnaire above was completed for a healthy 62-year-old Caucasian female born in 1963. The results indicated an 8.8% risk of major osteoporotic fracture (MOF) and a 1.5% risk of hip fracture. Since MOF is less than 20% and hip fracture is less than 3%, medications to treat OP may not be recommended by this patient’s physician.
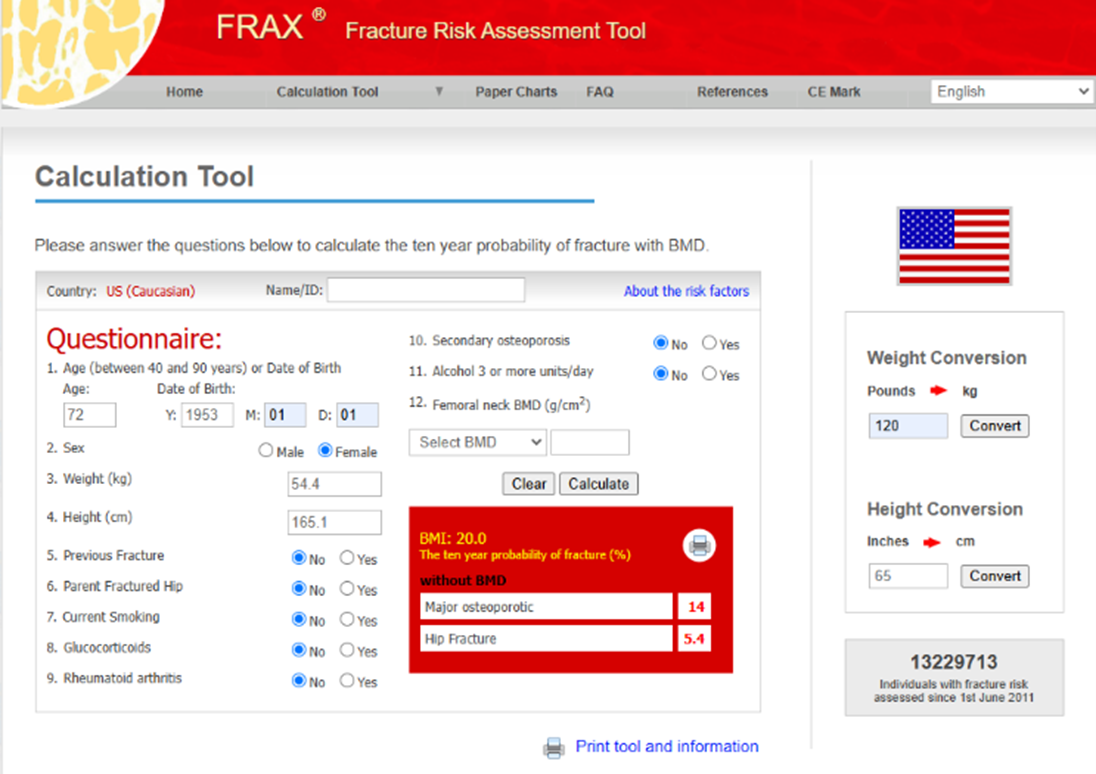
Let’s put a twist on FRAX and see how age input affects FRAX to demonstrate the bias of age on the database used in determining fracture risk. Let’s repeat the FRAX calculation at ten years older by changing the year of birth from 1963 to 1953. Go ahead, try this on your computer.
Then repeat the FRAX score using an age 10 years younger than the correct age (change from 1963 to 1973).
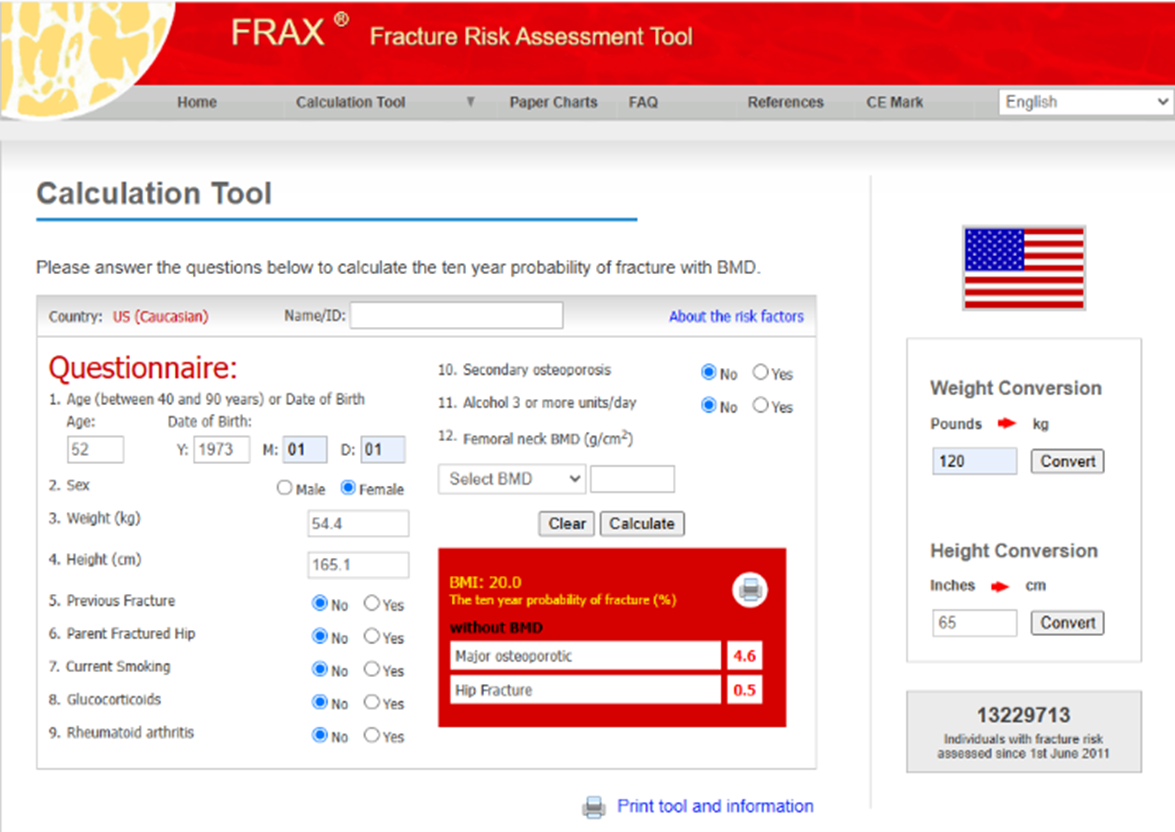
Each of the results are different. When age is increased, with no other CRFs being changed, MOF risk increases from 8.8% to 14% and hip fracture risk increases from 1.5% to 5.4%. When the age is decreased by 10 years, fracture risk of the spine decreases from 8.8% to 4.6% and hip fracture risk decreases from 1.5% to 0.5% with no changes in any other CRF.
The databases used by any method to determine fracture risk are designed for the general population. Age is a significant factor in determining fracture risk based on the statical assessment of the general population. We all know that the overall American population is not healthy. There are potentially many reasons for that but there is consensus that the average American diet is the reason most Americans suffer from many diseases as they get older. In addition, lack of activity and exercise, lifestyle choices (smoking and alcohol use) and stress ravage the body and bring about many diseases associated with age (heart disease, kidney disease, cancer, and osteoporosis, to list a few). Therefore, the databases represent an overall, unhealthy population, especially in the older age groups.
These current databases may not be particularly useful for individuals who are physiologically young because of healthy lifestyle choices. There is no appropriate database for physiologically young people. Fracture risk assessment tools including FRAX, REMS, and DXA do not know whether you are healthy or physiologically young. Whether you are healthy or not healthy, the information entered is what it is and therefore, each person’s fracture risk is estimated the same way, with the same level of risk being assigned.
In our experience with REMS, we have noticed that fracture risk may be overpredicted by REMS starting around age 66-67 years old. There are some attempts to try to address this issue, but there is no standardized method because the age-dependent database is universal. Even though there is concern that the absolute measurements may not be correct, REMS (and other methods) are still useful because the tests will establish a personal baseline which can then be used for comparison for future testing.
Remember, you are more than your T-score. You are an entire you! T-scores, Z-scores, BMD and Fragility Scores are pieces of the puzzle for your bone health, not the whole picture
Next in the series: Part 4: Risk and Odds…C’mon, what are the odds something bad will happen???








